Collected useful information on the Rh-conflict. The table is increasing
In the antenatal clinic, a pregnant woman must be checked for the Rh factor. If it is negative, it is necessary to determine the Rh affiliation of the father. At the risk of Rh-conflict (in the father - Rh +), the woman's blood is repeatedly examined for the presence of antibodies to fetal erythrocytes and their amount.
i note that it is absolutely not necessary that a Rh conflict will develop with an Rh-incompatible pregnancy. Very often, Rh-conflict pregnancy proceeds without any negative consequences for the fetus, since antibodies in the blood future mother they may not be produced at all, or they may be produced in a small amount that does not pose a danger to the child.
What are the factors that can contribute to the production of antibodies in the body of the expectant mother?
First factor capable of provoking the production of antibodies is the ingress of the baby's blood into the mother's bloodstream. This situation can occur during childbirth, abortion or miscarriage. The likelihood of developing antibodies during amniocentesis is also high. Amniocentesis is a test done by inserting a long needle through the abdominal wall into the uterus. Also, the ingress of "foreign" antibodies can occur through the placenta. The danger increases in the presence of increased placental permeability, due to infectious factors, minor injuries, hemorrhages.
Second factor The risk may be due to the fact that "hostile" antibodies have already been produced in the woman's body earlier, for example, during blood transfusion without taking into account Rh compatibility.
Third factor - this is a factor of surprise, because there is always the possibility that antibodies will begin to be produced in the body of a pregnant woman for no reason.
If the first encounter of the organism with foreign bodies has already occurred, then the “memory” of the organism will inevitably produce antibodies upon a repeated encounter with threatening agents. That is why the likelihood of Rh-conflict in the first pregnancy is relatively low and is only 10%. But, if you do not take the necessary preventive actions, then when a second pregnancy occurs, the likelihood of a Rh-conflict will increase significantly, since in any case, during childbirth, a Rh-positive child comes into contact with the Rh-negative blood of his mother.
By the level of antibodies in the blood of the expectant mother, the doctor can determine the possible onset of the Rh-conflict and draw conclusions about the alleged Rh factor in the child.
During the first pregnancy, the immune system of the expectant mother only "gets to know the strangers" (Rh + erythrocytes), little antibodies are produced and a conflict may not arise. However, “memory cells” remain in the woman’s body, which, in subsequent pregnancies, promptly “organize” the rapid and powerful production of antibodies against the Rh factor. Consequently, the risk of fetal injury increases with each subsequent pregnancy.
Therefore, immediately after childbirth, the Rh factor is determined in the baby. If it is positive, then the mother is injected with anti-Rh serum (anti-Rh immunoglobulin) no later than 72 hours after delivery, which will prevent the development of Rh-conflict during the next pregnancy.
The same prophylaxis with anti-rhesus serum Rh-negative women should be carried out after an ectopic pregnancy, abortion, miscarriage.
Carrying out Rh-conflict pregnancy
Fate has played a cruel joke on you, it so happened that you fall into the risk group. Don't worry, any problem is solvable, you just need to draw up a plan of action.
The first thing to do is to approach the issue of pregnancy planning responsibly. Namely, try to avoid situations that can provoke a Rh-conflict in the future, among them: abortion or miscarriage with a positive Rh factor in the fetus. If, nevertheless, the above situations occurred, you need to introduce a special drug as soon as possible, which will prevent the production of Rh antibodies.
It turns out that any termination of a "positive" pregnancy is fraught with subsequent serious consequences for the unborn child, because if antibodies have already been developed once, they will be produced again and again with each Rh-conflict pregnancy.
When the pregnancy has come, you need to try to register with the antenatal clinic as soon as possible, and immediately focus your gynecologist's attention on your particularity. The first and, perhaps, the most effective security measure in this case is the donation of blood for the presence of antibodies in it. This should be done throughout pregnancy: up to 32 weeks - 1 time per month, at 32-35 weeks 2 times a month, for the remaining period - weekly.
If everything is going well, and antibodies are not detected in the blood, then at 28 weeks the gynecologist may recommend to do a kind of "Rh - vaccination" - to introduce an anti-Rhesus immunoglobulin. Rh vaccination binds the baby's erythrocytes that have entered the mother's blood, thus eliminating the possibility of antibodies formation.
If the situation is critical and the antibody titer is significantly increased, then immediate hospitalization of the expectant mother and constant medical monitoring of her condition are necessary. Condition monitoring includes: tracking the dynamics of the titer of antibodies in the mother's blood, ultrasound research data, data from the study of amniotic fluid (amniocentesis) or the study of umbilical cord blood (cordocentesis).
If the pregnancy has reached full-term, a planned cesarean section is performed. If not, then you have to resort to intrauterine blood transfusion. Resolving childbirth with progressive Rh-conflict, as a rule, is carried out by caesarean section, this is done in order to isolate the baby from the source of "dangerous" antibodies as soon as possible.
With a favorable resolution of pregnancy, that is, if antibodies have not been developed, and the child has a positive Rh factor, you will definitely have to inject an anti-Rh - immunoglobulin in order to reduce the risk of Rh conflict in the next pregnancy. More precisely, such an injection should be given in the maternity hospital, but in order to protect both yourself and the unborn child, you should control this issue yourself, having agreed in advance with your doctor. In order to be completely confident and to exclude unforeseen situations, it is better to purchase this drug yourself and take it with you to the hospital.
Attaching the baby to the breast with Rh-conflict.
When the mother has a negative Rh, and the father is positive, it is possible to feed the child in the hospital if the pregnancy is the first or after the previous pregnancy an antiresus injection was given (anti-D immunoprophylaxis - author's note), explains GV consultant Anna Ilyina. “And here's why: antibodies in the blood (and milk) of such a mother appear only on the second or third day after childbirth, and if an anti-D injection is given, or the child turns out to be Resus-negative, then there will be no antibodies at all.”
“I would like to explain the position of official medicine in terms of early attachment to the breast of a newborn with a threat of Rh-conflict,” says neonatologist Sergei Gonchar. - The recommendation looks quite categorical - such a baby should receive his first feeding in the form of expressed donor milk. But, of course, modifications of this approach are quite acceptable. And this is very cool. The first pregnancy is not a 100% guarantee of the absence of anti-rhesus antibodies in the woman's body. Immunization ("active acquaintance" - Approx. Author) of a woman with Rh antigen could occur much earlier (with blood transfusion, sexual intercourse, problems with the placenta during this very pregnancy, etc. - Approx. Author).
It does not give a complete guarantee of safety and timely (no later than three days from the moment of delivery) an injection of anti-rhesus immunoglobulin given to a woman. Memory cells (a special family of lymphocytes) live for years and are able to quickly organize a violent immune response to the Rh antigen, even if there are a minimum of these same cells. The injection of specific immunoglobulin immediately after childbirth reduces the formation of memory cells, but cannot prevent the survival of the very minimum that will pose a danger to the baby in the next pregnancy.
Therefore, a guarantee of the safety of early attachment to the baby's breast from a Rh-negative mother is given only by one fact - a negative Rh-belonging of the baby himself. Theoretically, this is quite possible, but in practice it is checked in the first minutes after the birth of a child.
So, if a woman is Rh-negative, and her husband is Rh-positive, then in order to reasonably demand her baby for feeding right in the delivery room, it is highly desirable for mom to do the following:
if your pregnancy is the first one, then you still cannot neglect the regular examination of your blood for the content (titer) of anti-rhesus antibodies. Especially if you have ever received a blood transfusion;
if the pregnancy is not the first, then such a study is doubly relevant. It does not matter how the previous pregnancies ended - childbirth, miscarriages or abortions;
be sure to monitor the titer of these antibodies even if you have been injected with anti-rhesus immunoglobulin after a previous birth (abortion, miscarriage)
follow the recommendations of the obstetrician-gynecologist, which he gives according to the results of the examination of your blood;
ask doctors to determine the antibody titer on the last day before childbirth - according to the results of this study, it will be possible to more or less definitely judge the safety of early attachment to the breast. If antibodies are present, then feeding is already fraught with potential danger;
ask the doctor to determine the Rh-belonging of the baby immediately after birth, without delaying.
“If your baby is Rh-negative, you can safely apply it to the breast (of course, if there are no other contraindications),” summarizes the neonatologist Sergei Gonchar. - If he is Rh-positive, and during pregnancy (especially just before childbirth) you have not found anti-Rh antibodies, you can attach the baby to the breast, but with reasonable care. Although a newborn usually sucks a very small amount of milk during his first feeding, regular monitoring of the level of bilirubin, hemoglobin and red blood cells in his blood is necessary. With indications of a possible Rh-conflict, it is urgent to switch to feeding with donor milk. Finally, if anti-rhesus antibodies were detected in the mother's blood during pregnancy, early breastfeeding is contraindicated.
Once again, I would like to draw the attention of Rh-negative women - the absence of the aforementioned antibodies in your body should not be "proven" by theoretical calculations - there are objective research methods for this. And only with their help you can get a real idea of \u200b\u200bthe safety level of early breastfeeding of your baby. "
And what is the Rh-conflict dangerous for a child?
Once in the fetal bloodstream, immune Rh antibodies react with its Rh-positive erythrocytes (antigen-antibody reaction), resulting in destruction (hemolysis) of erythrocytes and the development of hemolytic disease of the fetus (HDN). The destruction of red blood cells leads to the development of anemia (a decrease in the amount of hemoglobin) in the fetus, as well as damage to its kidneys and brain. As red blood cells are continuously destroyed, the fetal liver and spleen try to speed up the production of new red blood cells, while increasing in size. The main manifestations of fetal hemolytic disease are an increase in the liver and spleen, an increase in the amount of amniotic fluid, and a thickening of the placenta. All of these signs are detected using ultrasound during pregnancy. In the most severe cases, when the liver and spleen cannot cope with the load, severe oxygen starvation occurs, hemolytic disease leads to intrauterine fetal death at various stages of pregnancy. Most often, the Rh-conflict manifests itself after the birth of a child, which is facilitated by the entry of a large amount of antibodies into the baby's blood when the integrity of the placenta vessels is disturbed. Hemolytic disease is manifested by anemia and jaundice of newborns.
Depending on the severity of hemolytic disease, several forms are distinguished.
Anemic form is the most benign variant of HDN course. It manifests itself immediately after birth or during the 1st week of life with anemia associated with pallor skin... The size of the liver and spleen increases, there are small changes in the test results. The general condition of the baby is disturbed little, the outcome of this course of the disease is favorable.
Icteric form This is the most common moderate form of HDN. Its main manifestations are early jaundice, anemia and an increase in the size of the liver and spleen. The baby's condition worsens with the accumulation of the decay product of hemoglobin - bilirubin: the baby becomes lethargic, drowsy, his physiological reflexes are inhibited, and muscle tone decreases. On the 3-4th day without treatment, the level of bilirubin can reach critical levels, and then symptoms of nuclear jaundice may appear: stiff neck, when the baby cannot tilt his head forward (attempts to bring the chin to the chest are unsuccessful, they are accompanied by crying), convulsions, wide open eyes, shrill scream. By the end of the 1st week, bile stagnation syndrome may develop: the skin becomes greenish, feces become discolored, urine darkens, the content of bound bilirubin increases in the blood. The icteric form of HDN is accompanied by anemia.
The edematous form is the most severe variant of the course of the disease. When early development immunological conflict, miscarriage may occur. With the progression of the disease, massive intrauterine hemolysis - the breakdown of red blood cells - leads to severe anemia, hypoxia (oxygen deficiency), metabolic disorders, a decrease in the level of proteins in the bloodstream and tissue edema. The fetus is born in an extremely serious condition. The tissues are edematous, fluid accumulates in the body cavities (chest, abdominal). The skin is sharply pale, glossy, jaundice is poorly expressed. Such newborns are lethargic, their muscle tone is sharply reduced, reflexes are depressed.
The liver and spleen are significantly enlarged, the abdomen is large. Expressed cardiopulmonary insufficiency.
Treatment of HDN is aimed primarily at combating high levels of bilirubin, elimination of maternal antibodies and elimination of anemia. Moderate and severe cases are subject to surgical treatment. Surgical methods include replacement blood transfusion (BCT) and hemosorption.
ZPK still remains an indispensable intervention in the most severe forms of HDN, as it prevents the development of nuclear jaundice, in which the nuclei of the fetal brain are damaged by bilirubin, and restores the number of blood cells. The ZPC operation consists in taking blood from a newborn and transfusing it into the umbilical vein with donor Rh-negative blood of the same group as the blood of the newborn). Up to 70% of the baby's blood can be replaced in one operation. Blood transfusion is usually carried out in the amount of 150 ml / kg of the child's body weight. With severe anemia, a blood product is transfused - erythrocyte mass. The ZPC operation is often repeated, up to 4-6 times, if the bilirubin level again begins to reach critical levels.
Hemosorption is a method of extracting antibodies, bilirubin and some other toxic substances from the blood. In this case, the baby's blood is taken and passed through a special apparatus, in which the blood passes through special filters. The "purified" blood is poured into the baby again. The advantages of the method are as follows: the risk of transmission of infections with donor blood is excluded, the baby is not injected with a foreign protein.
After surgical treatment or in the case of a milder course of HDN, transfusions of solutions of ALBUMIN, GLUCOSE, HEMODESIS are performed. In severe forms of the disease, intravenous administration of PREDISOLONE for 4-7 days has a good effect. In addition, the same methods are used as for transient conjugative jaundice.
The method of hyperbaric oxygenation (HBO) has found very wide application. Pure humidified oxygen is supplied to the pressure chamber where the baby is placed. This method allows you to significantly reduce the level of bilirubin in the blood, after which the general condition improves, the effect of bilirubin intoxication on the brain decreases. Usually 2-6 sessions are carried out, and in some severe cases, 11-12 procedures are required.
And at the present time the question of the possibility and expediency of breastfeeding babies with the development of HDN. Some experts consider it to be quite safe, while others are inclined in favor of canceling breastfeeding in the first week of a baby's life, when its gastrointestinal tract is most permeable to immunoglobulins and there is a danger of additional ingestion of maternal antibodies into the baby's bloodstream.
Of personal experience I can advise you to discuss with the child's doctor the delay of hepatitis vaccination even before birth, because it is difficult, for a child with Rh-conflict in general, a separate consultation and the schedule of vaccinations is important.
Second and subsequent pregnancies.
If the rhesus conflict during the first pregnancy passed you, the injection of immunoglobulin was injected on time, then during the second pregnancy for you initially it will not differ from the first, i.e. the likelihood of developing Rh conflict during pregnancy will still remain at the level of 10%.
To prevent Rh-conflict and hemolytic disease during the second pregnancy, a woman is given a series of injections, which should be given as soon as antigens are detected in the blood. In some cases, antigens can be observed in the blood already from the ninth week of pregnancy, which must be taken into account when choosing a therapy for the mother. Those mothers who have infectious processes that violate the placental barrier, minor hemorrhages and trauma to the placenta are at greater risk.
But in any case, it is important to remember: the very fact of the possibility of a Rh conflict during pregnancy and even the presence of antibodies in the blood is not a contraindication to pregnancy, and even less a reason for its termination. It's just that such a pregnancy requires a much more responsible and attentive attitude towards oneself. Try to find a competent specialist whom you completely trust, and strictly follow all his recommendations.
Pregnancy with titer
so far, from everything I read on this topic, I realized that such Bs are in control. if antibodies appear, then amniocentesis and cordocentesis are performed, ultrasound is additional to control the size of the child's liver and polyhydramnios in the mother. Childbirth is most often carried out by cesarean, in order to reduce the risk of injury. Often the issue of childbirth is raised at 34 weeks. And such women should give birth in RD with children's intensive care, tk. if there is a complicated pregnancy, then the likelihood of HMB is very high, and as a rule, then a blood transfusion is often necessary for a child. Well, from therapy, only if something is prescribed for bilirubin, well, droppers.
Because There is a risk of antibodies with B, but there is also the fact that they will not appear, then it is worth taking care of controlling the titer and buying an anti-rhesus immunoglobulin, if it can still be administered by the time.
This is from a good article:
Management tactics
A blood test for anti-rhesus antibodies is carried out for all pregnant women at the first visit to a doctor. For Rh-negative women, the study is repeated at 18-20 weeks, and then monthly. Before the 20th week of pregnancy, isoimmunization rarely develops, usually after the 28th week of pregnancy. This explains the timing of anti-Rh0 (D) -immunoglobulin administration.
Rh-negative women who are pregnant with an Rh-positive fetus are given anti-Rh0 (D) -immunoglobulin at 28 weeks. This drug must also be prescribed before amniocentesis. The risk of isoimmunization is highly dependent on the method of delivery. In childbirth, the dose of anti-Rh0 (D) -immunoglobulin is selected depending on the results of the examination of the maternal blood smear, stained according to Kleihauer-Betke.
The severity of hemolytic disease of the newborn.
At present, it is not finally decided whether the number of pregnancies accompanied by isoimmunization affects the severity of hemolytic disease of the newborn. In the first pregnancy with isoimmunization, fetal dropsy develops in about 8% of cases. Unfortunately, it is impossible to predict its occurrence in subsequent pregnancies. To assess the condition and prognosis of pregnancy in a woman with Rh-negative blood, it is not enough to determine the titer of anti-Rh antibodies.
Lily's chart.
In 1961, Lily proposed a special method for assessing the data of the spectrophotometric study of amniotic fluid obtained by amniocentesis.
It was found that the most accurate content in amniotic fluid bilirubin and, accordingly, the severity of hemolytic disease reflects the optical density of the amniotic fluid, determined by passing light with a wavelength of 450 nm. When constructing her chart, Lily used data from research conducted in different terms pregnancy in 101 women with isoimmunization.
Three zones are distinguished on the diagram, corresponding to three degrees of severity of hemolytic disease. Severe hemolytic disease corresponds to zone 3. This condition is often accompanied by dropsy of the fetus. The child is usually not viable. Mild hemolytic disease corresponds to zone 1. In recent years, some changes have been made to the Lily chart, as a result of which its diagnostic and predictive accuracy has increased.
Delivery.
In 50-60% of pregnant women with isoimmunization, there are no indications for amniocentesis, or the optical density of amniotic fluid does not exceed the average values \u200b\u200bof zone 2 on the Lily chart. In such cases, independent childbirth is allowed. If at 35-37 weeks of pregnancy the optical density corresponds to the upper border of zone 2 or has higher values, delivery is performed at 37-38 weeks. Pre-determine the degree of maturity of the lungs of the fetus. In the presence of dropsy of the fetus and a gestational age of more than 34 weeks (20% of all cases of dropsy of the fetus), delivery is carried out immediately, as soon as the optical density indicator reaches the upper border of zone 2. The maturity of the fetal lungs is preliminarily determined. Corticosteroids are given to accelerate maturation about 48 hours before delivery.
Treatment
If the risk of prematurity is high, delivery is postponed and intrauterine treatment of hemolytic disease is performed.
Intrauterine blood transfusion was suggested by Lily in 1963. He used the method of intraperitoneal transfusion. With the advent of ultrasound, intravascular blood transfusion became possible: since 1981 with the help of fetoscopy, and since 1982 - by cordocentesis. Intrauterine blood transfusion is a dangerous procedure for both the fetus and the pregnant woman, therefore it must be performed by an experienced doctor. Research has shown that most babies who have had intrauterine blood transfusions grow and develop normally. Deviations were noted in cases when hemolytic disease was combined with deep prematurity.
Anti-Rh0 (D) -immunoglobulin is administered after childbirth as soon as the Rh factor is determined in the study of umbilical cord blood. If anti-Rh0 (D) -immunoglobulin is not administered within 72 hours after delivery, it is certainly administered no later than two weeks after delivery. With a delay, the effectiveness of prevention decreases.
The dose of anti-Rh0 (D) -immunoglobulin is calculated depending on the volume of fetal-maternal transfusion, which is estimated by counting fetal erythrocytes in a mother's blood smear, stained according to Kleihauer-Betke. If the volume of fetal-maternal transfusion does not exceed 25 ml, 0.3 mg of anti-Rh0 (D) -immunoglobulin is injected intramuscularly, with a transfusion volume of 25-50 ml - 0.6 mg, etc.
The overwhelming majority of young expectant mothers have a poor idea of \u200b\u200bwhat is meant by the term "Rh factor" and why this parameter is so important.
Rhesus is a protein found on the surface of red blood cells. It is present in about 85% of the world's inhabitants.
How does the Rh conflict arise?
The main reason for the development of the Rh-conflict is the discrepancy between these characteristics of the blood of the mother and the unborn child, i.e. if the baby's blood is positive, and his mother's is negative. In this case, the Rh-conflict for blood groups does not occur.
The mechanism of development of this phenomenon is as follows. At the moment when the erythrocytes of the fetus with rhesus proteins enter the blood of the expectant mother through the vessels of the placenta, they are perceived as foreign. As a result, the immune system of the pregnant woman's body is activated, which is accompanied by the production of antibodies, which are designed to destroy the fetal blood cells that do not correspond to the mother's cells.
Due to the fact that the baby's erythrocytes are periodically destroyed, his spleen and liver, as a result of increased production of blood cells, increase in size.
As a result, the baby's body cannot cope, a strong one sets in, which can lead to death.
In what cases is Rh-conflict possible?
In order to avoid such a situation, a girl should know the Rh factor of her lover even before marriage. Violation occurs in cases where the wife has no Rhesus protein, and the husband has it. In such a situation, in 75% of cases, there is a discrepancy.
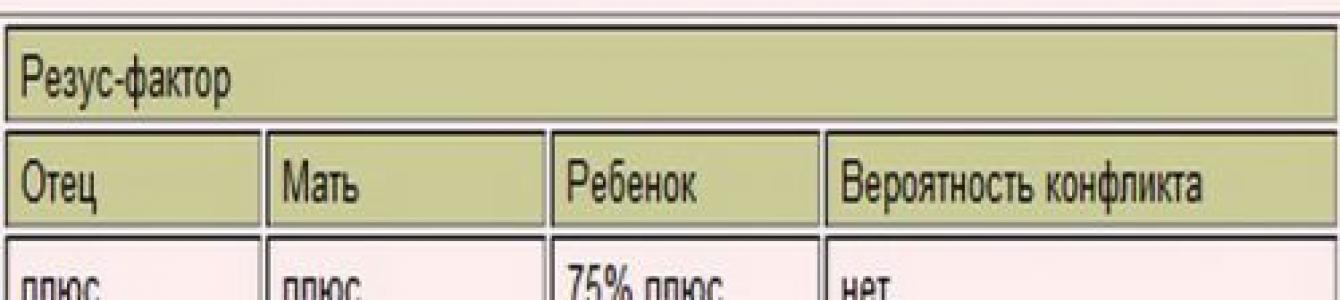
Therefore, in order to prevent the development of Rh-conflict, a table of the probability of occurrence of violations during pregnancy was compiled.

What are the signs of this disorder?
There are no clinical signs of the development of Rh-conflict during pregnancy, i.e. the pregnant woman is not able to independently determine the violation. This is done using an ultrasound scan.
So, the symptoms of this disorder may be:
- the development of puffiness, which is accompanied by the accumulation of fluid in the body cavities;
- an increase in the size of the fetal body;
- pose of "Buddha" (baby's legs are set aside, due to a strong increase in the abdomen);
- enlargement of the spleen and liver of the fetus;
- swelling and thickening of the placenta.
Is pregnancy possible in
Do not despair if a girl has Rh negative blood, and her chosen one has positive blood. As a rule, the first pregnancy is normal. This is explained by the fact that a woman's body first encounters Rh-positive blood, and little antibodies are produced. In cases where there were many blood cells with Rhesus protein in the mother's body, the so-called memory cells remain in her blood, leading to a conflict during the second pregnancy.
How is Rh-conflict prevention carried out?
With an already onset pregnancy, special attention is paid to the prevention of Rh-conflict.
So, first of all, they check whether this protein is present in the mother's blood. If he is not, then the father is subjected to a similar procedure. If it contains rhesus, then the blood of the expectant mother is subjected to a thorough examination for the presence of antibodies in it. At the same time, the level of these formations in the blood of a pregnant woman is constantly monitored. So, up to 32 weeks, the analysis is carried out once a month, and in the period 32-35 weeks - 2 times every 30 days.
After the baby is born, blood is taken from him, in which rhesus is determined. If it is positive, then within 3 days the mother is injected with serum - immunoglobulin, which prevents the occurrence of a conflict during the next pregnancy.
What are the consequences of the Rh-conflict?
A Rh-conflict detected in time, as a rule, does not have negative consequences. However, this is not always the case. If a miscarriage occurs, then sensitization (production of antibodies) occurs in only 3-4% of cases, during medical abortion - 5-6%, after normal childbirth - 15%. In this case, the risk of sensitization increases with placental abruption and caesarean section.
As everyone knows from time immemorial school times, "Rhesus" is such a monkey. It was in her blood that a certain "factor" was found in the first, which was named in her honor.
Those of our readers who had a solid A at the school in biology and their mother still has a certificate of honor from a meeting of young anatomy lovers in the mezzanine, know that this “factor” is actually Rh proteins, located on the surface of erythrocytes. And some people have these proteins on erythrocytes, while others are completely absent.
The presence or absence of the Rh factor in the erythrocytes of people determines their belonging to rh positive or rh negative group. It is found that 86% of people of the Caucasian ("white") race have a positive Rh factor, and 14% - negative.
Rhesus antigens are produced in the fetus, starting from 8-10 weeks of intrauterine development.
When does Rh-conflict arise?
Rhesus conflict may occur during pregnancy if the mother's Rh factor does not match the fetus's Rh factor. When, when a baby is a carrier of a positive Rh factor, the likelihood of a Rh-conflict is much higher than in the opposite situation, and its consequences are much more serious. Therefore, most often, when it comes to rh-conflict pregnancy, the combination "Rh-negative mother + Rh-positive baby" is meant.
Such a combination occurs in about 75% of cases, when mom is Rh negative, dad is Rh positive (for our especially curious readers, a short excursion into genetics: the genotype responsible for the positive daddy Rh factor can be homozygous or heterozygous. In case of homozygosity of the daddy Rh factor future baby will necessarily be Rh-positive, otherwise the chances of giving birth to a "positive" and "negative" baby are equal).
What is risk of Rh-incompatible pregnancy? The fact is that if Rh-positive erythrocytes get into the blood of a Rh-negative person, the body will perceive them as something foreign, and will begin to produce antibodies that destroy "strangers". And if, for any reason, such antibodies appear in the mother's blood, the unborn child will be in serious danger.
Once through the placenta into the bloodstream of the child, antibodies begin to destroy his red blood cells. The severity of the consequences of this is easy to imagine: after all, we all know from school that the most important function of red blood cells is to transport oxygen to organs and tissues. The pathological condition of the fetus, resulting from the ingestion of Rh antibodies into its blood, doctors call hemolytic disease... Let's not dwell on detailed descriptions the symptoms and outcomes of this disease - I think, and so the scale of the consequences caused by the catastrophic lack of oxygen, and even in a just forming organism, is approximately clear!
But in fact, it is not at all necessary that with an Rh-incompatible pregnancy, a Rh-conflict between the mother and the fetus will develop. Very often, during such a pregnancy, antibodies are either completely absent in the blood, or their amount is so small that it does not pose a serious danger to the child.
What factors can trigger the production of antibodies in the body of the expectant mother?
- The entry of the baby's blood into the mother's bloodstream. This can happen during childbirth, abortion or spontaneous miscarriage, during amniocentesis (a study performed by inserting a long thin needle through the abdominal wall into the uterus), etc. In addition, the ingestion of foreign red blood cells can occur intrauterinely through the placenta. Their penetration into the maternal bloodstream is facilitated by infectious factors that increase the permeability of the placenta, minor injuries, hemorrhages and other damage to the placenta.
- Antibodies in the blood of a Rh-negative woman had already been developed sometime before pregnancy as a result, for example, of blood transfusion without taking into account Rh compatibility (even if at an early age).
- In a very small percentage of cases, antibodies to Rh-positive red blood cells are formed in the body of a pregnant woman for no apparent reason.
After the first meeting of the body with foreign erythrocytes has occurred, "memory cells" remain in the woman's blood, which, in subsequent collisions with "enemy" blood cells, organize the rapid production of antibodies. That is why the likelihood of Rh-conflict during the first pregnancy is relatively low (about 10%), but if you do not take certain preventive measures, then in subsequent pregnancies, the likelihood of problems increases significantly, since during the delivery of a Rh-positive child, contact with incompatible blood occurs ...
What to do?
So, by the will of fate, it turned out that, if you believe all of the above, you have the likelihood of a Rh-conflict pregnancy. What is the plan of action?
First, you need the most careful approach to planning pregnancy.The fact is that it is very important for you to avoid cases of "collision" with Rh-incompatible blood (and this can happen, in particular, during an abortion or miscarriage, if the fetus was Rh-positive). In such cases, it is necessary to introduce a special drug as soon as possible to prevent the production of Rh antibodies.
Thus, any termination of pregnancy is associated with a very high risk for you. After all, if antibodies have already been developed once, they will be produced again and again with each Rh-incompatible pregnancy, posing a serious threat to the health of the little man.
After pregnancy you need to register with the antenatal clinic as early as possible, focusing the attention of your gynecologist on this extremely important feature of your pregnancy at the very first appointment. The first safety measure in this case is the regular donation of blood for antibodies throughout the entire period of pregnancy (up to 32 weeks - once a month, from 32 to 35 weeks - 2 times a month, and then weekly).
If everything goes smoothly and antibodies in the blood of the expectant mother are not detected, at the 28th week of pregnancy, the doctor may recommend the prophylactic administration of anti-Rhesus immunoglobulin, which is a kind of "Rh vaccine" - it binds the baby's erythrocytes that have entered the mother's blood and thus does not allow an immune response (formation of antibodies).
With a critical increase in the antibody titer, the expectant mother needs to be hospitalized in a specialized perinatal center, where the condition of the mother and baby will be monitored constantly. Doctors will track:
- The dynamics of the titer of antibodies in the blood of the expectant mother;
- Ultrasound data: an increase in the size of the fetal liver, thickening of the placenta, the appearance of polyhydramnios and fluid in the pericardium and abdominal cavity of the fetus;
- Data of amniocentesis (examination of amniotic fluid) or cordocentesis (examination of umbilical cord blood).
If the pregnancy can be brought to full-term, then a planned cesarean section is performed. If not, you have to resort to intrauterine blood transfusion. Childbirth in situations where the Rh-conflict has arisen and progresses, most often occurs through a cesarean section, because it is necessary to isolate the baby from the source of destructive antibodies as early as possible.
And of course after the baby is born if the pregnancy has passed without the production of antibodies and the baby's Rh factor is positive, within 24-48 hours after the birth, you will be given anti-Rh immunoglobulin injectiondesigned to bind hostile Rh-positive red blood cells and prevent the production of antibodies (otherwise, the risk of complications during the next pregnancy will seriously increase). More precisely, an injection MUST be made in the maternity hospital, but in practice it will not be superfluous to discuss this moment with the doctors before childbirth and, if possible, control the timely administration of the drug after the baby is born. For complete confidence, it is best to buy this drug yourself at the pharmacy and take it with you to the hospital.
…what next?
If in the first Rh-incompatible pregnancy, the problem of antibody production has passed you, the injection of immunoglobulin is injected on time, then the next pregnancy for you will initially be no different from the first, i.e. the likelihood of developing Rh-conflict will still remain at the level of 10%.
But in any case, it is important to remember: the very fact of the possibility of a Rh conflict and even the presence of antibodies in the blood is not a contraindication to pregnancy, and even more so not a reason for terminating it. It's just that such a pregnancy requires a much more responsible and attentive attitude towards oneself. Try to find a competent specialist whom you fully trust, and strictly follow all his recommendations.
Afterword
So, in this article, we examined in detail the blood conflict when a mother with a negative Rh factor is pregnant with a Rh-positive child. This is the most common and dangerous case of conflict, but do not forget that conflicts are possible not only with Rh factor, but also with group incompatibility blood of mother and fetus. Therefore, when preparing for conception and registering for pregnancy in an antenatal clinic, do not refuse the appropriate tests and ask the doctor to comment on whether there is a danger of conflict in your particular situation. After all, mother's awareness and correct observation of a "conflict" pregnancy will allow your baby to be born healthy, and you will have many more children in the future!
Discuss in the forum:
Rh-conflict during pregnancy: what to do for a woman with a negative Rh factor to avoid the consequences
Rh-conflict during pregnancy arises as a result of blood incompatibility according to the Rh system (rhesus). According to statistics, this type of incompatibility occurs in 13% of married couples, but immunization during pregnancy occurs in 1 in 10-25 women.
Pregnancy of a woman with a negative Rh factor, in which the fetus has a positive Rh factor, leads to the development of antibodies by the mother's immune system to the baby's red blood cells.
As a result, fetal erythrocytes "stick together" and are destroyed. This is a humoral immune response to the presence of a protein foreign to the maternal organism, the Rh factor.
- Rh factor - what is it
- The likelihood of developing Rh-conflict during pregnancy: table
- The reasons
- Feto-maternal transfusion
- Rh-conflict during pregnancy: mechanism of occurrence
- Consequences for the child
- Risks
- Diagnostics, symptoms and signs of Rh-conflict during pregnancy
- Treatment
- Plasmapheresis for Rh-conflict pregnancy
- Cordocentesis
- Immunoglobulin with negative rhesus
- Can the Rh factor change during pregnancy?
What is Rh factor
To understand what Rh-conflict is during pregnancy, you need to dwell in more detail on such a concept as the Rh factor.
Rh (+) is a special protein - agglutinogen - a substance that can stick together red blood cells and damage them when they encounter an unfamiliar immune agent.

The Rh factor was first discovered in 1940. There are about 50 types of Rhesus antigens. The most mutagenic dominant antigen is the D antigen, which is found in the blood of 85% of people.
Antigen C is found in 70% of people, and antigen E is found in 30% of people on the planet. The presence of any of these proteins on the erythrocyte membrane makes it Rh positive Rh (+), the absence - Rh negative Rh (-).
The presence of agglutinogen D is of ethnicity:
- among people of Slavic nationality, 13% are Rh-negative people;
- among Asians 8%;
- in people of the black race, there are practically no people with Rh negative blood factor.
Recently, women with negative blood Rh factor have been increasingly encountered, according to the literature, this is associated with mixed marriages. Consequently, the frequency of Rh-conflict during pregnancy in the population increases.
System D antigen inheritance
The types of inheritance of any trait are divided into homozygous and heterozygous. For example:
- DD - homozygous;
- Dd - heterozygous;
- dd is homozygous.
Where D is the dominant gene and d is the recessive one.
Rh-conflict during pregnancy - table
If the mother is Rh positive, the father is Rh negative, then one of the three children will be born Rh negative with a heterozygous type of inheritance.
If both parents are Rh negative, then their children will have a negative Rh factor in 100%.
Table 1. Rh-conflict during pregnancy
| The man | Woman | Child | The likelihood of Rh-conflict during pregnancy | |
| + | + | 75% (+) | 25% (-) | Not |
| + | — | 50% (+) | 50% (-) | 50% |
| — | + | 50% (+) | 50% (-) | Not |
| — | — | 100% (-) | Not | |
The reasons
The reason for the Rh-conflict during pregnancy is:
- transfusion of incompatible blood according to the AB0 system - is extremely rare;
- fetal-maternal transfusion.
What is Feto-Maternal Transfusion?
Normally, during any pregnancy (physiological or pathological), a small number of fetal blood cells enter the mother's bloodstream.

A negative Rh factor during pregnancy in a woman is definitely dangerous for a baby with a positive Rh factor. Rhesus conflict develops, as well as any immunological reaction. At the same time, the first pregnancy can proceed without complications, but subsequent (second and third) pregnancies lead to Rh-conflict and severe symptoms of hemolytic disease of the fetus and newborn.
The mechanism of immunization (development of rhesus conflict)
Rh-negative mother and Rh-positive fetus exchange blood cells, the mother's immune system perceives the baby's red blood cells as foreign proteins and begins to produce antibodies against it. For the development of a primary immune response, 35-50 ml of fetal erythrocytes enter the mother's bloodstream.
The volume of blood that comes from the baby's bloodstream to the mother increases during obstetric invasive procedures, caesarean section, childbirth, and other obstetric manipulations.
The first immune response begins with the appearance of immunoglobulins M - these are large pentagram molecules (polymers) that hardly penetrate the placental barrier and do not destroy the fetal erythrocytes, thus cannot harm it. Therefore, the first pregnancy most often proceeds without consequences.
Secondary placental transfusion has consequences for the child. It occurs during repeated (second, third, fourth) pregnancy.

In the body of a pregnant woman, cellular memory works and, as a result of repeated contact with the Rh factor protein, protective antibodies are produced - immunoglobulins G - a Rh conflict develops. Immunoglobulin G molecules are small monomers that can penetrate the placental barrier and cause hemolysis - the destruction of fetal and newborn erythrocytes.
What contributes to the development of Rh sensitization?
The first pregnancy in an Rh-negative mother with an Rh-positive fetus in most cases ends well and ends with the birth of the fetus. Any subsequent pregnancy, regardless of outcome (miscarriage due to early dates, abortion, spontaneous interruption) in a Rh-negative woman becomes an impulse for the development of a secondary immune response and the appearance of immunoglobulins that destroy the baby's erythrocytes in utero.

The reason for the Rh-conflict during pregnancy in a Rh-negative mother can be:
- In the first trimester:
- medical abortion (surgical or medical), provided that these complications arose within 7-8 weeks.
According to the definition, Rh immunization (Rh sensitization / Rh conflict) is the appearance of Rh antibodies in a pregnant woman in response to fetal erythrocyte antigens entering the bloodstream, that is, to paraphrase it simply - it is the incompatibility of a mother with a Rh negative blood group with a child with a Rh positive blood group (and not with a husband, as many think).
Rhesus antigen is a protein found in the membrane of the red blood cells / red blood cells of most people. The blood of such people is Rh positive, and the blood of those who do not have this protein, respectively, is called Rh negative. About 1/3 of the population is Rh negative.
Rh-positive parents may well have a Rh-negative baby. In this case, a very peaceful, conflict-free relationship develops between the "positive" mother and her "negative" child: such a combination does not threaten either the woman or the fetus.
If the mother and father of the child have a Rh negative blood group, the child also has a negative Rh factor.
But if the mother has Rh-negative blood, and the father has positive, Rh-positive fetus occurs in 60% of pregnant women, but only 1.5% of these pregnancies develop incompatibility.
As a rule, with repeated pregnancy, the likelihood of incompatibility is higher than with the first.
The mechanism of development of the Rh-conflict
If Rh-positive erythrocytes meet with Rh-negative, then they stick together - agglutination. To prevent this from happening, the immune system of the Rh-negative mother produces special proteins - antibodies that bind to the Rh protein in the membrane of the fetal red blood cells (antigens), preventing them from sticking to the mother's own red blood cells. Antibodies are called immunoglobulins and are of two types: IgM and IgG.
The contact of fetal red blood cells with antibodies occurs in the space between the wall of the uterus and the placenta. At the first meeting of fetal Rh-positive erythrocytes with the immune system of a Rh-negative mother, IgM is produced, the size of which is too large to penetrate the placental barrier. That is why, as a rule, during the first pregnancy of a Rh-negative mother with a Rh-positive fetus, the conflict arises relatively rarely. Incompatibility develops when fetal antigens (Rh positive erythrocytes) re-enter the bloodstream of a Rh-negative mother, whose immune system then massively produces IgG, which, being smaller, penetrate the placenta and cause hemolysis, i.e. destruction of fetal red blood cells. This is how hemolytic disease of the fetus / newborn develops.
Complications of Rh-conflict
As a result of the destruction of erythrocytes, toxic damage occurs to almost all organs and systems of the fetus by the breakdown product of hemoglobin, a substance that is contained in erythrocytes and is responsible for oxygen transport. This is due to the decay product, bilirubin. First of all, the central nervous system of the fetus, liver, kidneys and heart is affected, fluid accumulates in its cavities and tissues, which interferes with the normal functioning of organs and systems up to intrauterine death in severe cases. It is in connection with such "rejection" of the fetus that Rh-negative mothers often develop the threat of miscarriage, and the risk of intrauterine fetal death increases.
Rh factors for Rh-conflict
Are divided into:
1. Pregnancy-related:
- any type of abortion: miscarriage, instrumental and medical abortion;
- ectopic pregnancy;
- childbirth, namely, in the third period, when the placenta is separated from the uterine wall;
- complication of pregnancy or childbirth - premature placental abruption, which is accompanied by bleeding from the vessels of the placenta;
- any invasive research methods: (amniocentesis, cordocentesis - puncture of the fetal bladder or umbilical cord).
2. Unrelated to pregnancy:
- immunization with blood transfusion;
- using one needle for intravenous drug use.
Rh-conflict symptoms
The patient has no clinical manifestations, her condition does not suffer.
Symptoms of hemolytic disease in the fetus during pregnancy can only be detected by ultrasound, they are: swelling, accumulation of fluid in the cavities (abdominal, chest, in the cavity of the pericardium); due to the accumulation of fluid in the abdominal cavity of the fetus, the size of the tummy increases, the fetus takes a certain position "Buddha pose" (when, unlike the norm, the limbs are removed from the enlarged tummy), an increase in the size of the liver and spleen, an increase in the size of the heart, a "double" contour appears heads (as a result of swelling of the soft tissues of the head). Also, edema is determined and, accordingly, a thickening of the placenta and an increase in the diameter of the umbilical vein. Depending on the predominance of a particular symptom, three forms of hemolytic disease of the fetus are distinguished: edematous, icteric and anemic.
Diagnosis of Rh-conflict and pregnancy management tactics
The purpose of monitoring pregnant women during Rh immunization is: examination to detect sensitization, prevention of Rh immunization, early diagnosis of hemolytic disease of the fetus and its correction, as well as determination of the most optimal timing for delivery. When registering for pregnancy, the determination of the blood group is shown, both for the pregnant woman herself and the father of the child in a planned manner. In the presence of Rh-negative blood in the mother and Rh-positive blood in the father, pregnant women undergo a blood test for antibodies once a month, monitoring the dynamics of the antibody titer. In the presence of any antibody titer, pregnancy is considered Rh sensitized. If antibodies are detected for the first time, then their class is determined (IgM or IgG). Further, a blood test for antibodies is carried out monthly, observing the patient for up to 20 weeks in an antenatal clinic, and after 20 weeks, they are sent to specialized centers to determine further management tactics, possibly, to conduct treatment and decide on the method and timing of delivery.
Starting at 18 weeks, the fetus is assessed using an ultrasound scan.
Methods for assessing the condition of the fetus are divided into:
1. Non-invasive methods.
- Ultrasound, which assesses: the size of the fetal organs, the presence of free fluid in the cavities, the presence of edema, the thickness of the placenta and the diameter of the umbilical vein. The first ultrasound is performed at 18-20 weeks, repeated at 24-26 weeks, 30-32 weeks, 34-36 and immediately before delivery. Depending on the severity of the fetus, it is possible to conduct this study more often, up to daily (as, for example, after a blood transfusion to the fetus).
- dopplerometry, which assesses the functional parameters of the heart, blood flow velocity in large vessels of the fetus and the umbilical cord, etc.
- cardiotocography assesses the reactivity of the fetal cardiovascular system, reveals the presence or absence of hypoxia (lack of oxygen).
2. Invasive:
- amniocentesis - puncture of the fetal bladder for the purpose of taking amniotic fluid to assess the severity of hemolysis by the content of bilirubin (a breakdown product of hemoglobin), which is one of the most accurate methods for assessing the severity of the fetus. Unfortunately, this method is fraught with many complications: infection, prenatal rupture of amniotic fluid, premature birth, bleeding, premature placental abruption. Indications for amniocentesis: antibody titer 1:16 or more, the patient has children who have had a severe form of hemolytic disease of the newborn.
- cordocentesis - puncture of the umbilical cord for the purpose of blood sampling. The method allows you to accurately assess the severity of hemolysis, to simultaneously carry out intrauterine blood transfusion to the fetus. In addition to those complications that are characteristic of amniocentesis, with cordocentesis, it is also possible to develop a hematoma of the umbilical cord and bleeding from the puncture site. Indications for cordocentesis are to determine the signs of hemolytic disease of the fetus by ultrasound, the antibody titer is 1:32 and higher, the patient has children who have undergone severe form of HDP in the past or died from it, high levels of bilirubin in the amniotic fluid obtained during amniocentesis.
Due to the possible risk, before carrying out either procedure, the patient must be informed by the doctor about the possibility of adverse consequences of the procedure and give his written consent to its conduct.
Treatment of Rh-conflict
In modern obstetrics, the only method of treatment with proven efficacy is intrauterine blood transfusion, which is carried out with severe anemia (anemia) in the fetus. This kind of treatment is carried out only in a hospital and allows you to achieve a significant improvement in the condition of the fetus and reduce the risk of premature birth and the development of a severe form of the disease after birth.
High-risk patients (in whom the antibody titer was detected in the early stages, those with the antibody titer 1:16 and higher, those who had a previous pregnancy with Rh conflict) are observed in the antenatal clinic for up to 20 weeks, and then sent to specialized hospitals for the above treatment.
Various methods of purifying the mother's blood from antibodies (plasmapheresis, hemosorption), methods affecting the activity of the immune system (desensitizing therapy, immunoglobulin therapy, transplanting a skin flap of the child's father to the patient) are currently considered ineffective or even ineffective.
But, unfortunately, despite significant advances in the field of correcting the state of the fetus, the most effective way is the cessation of the supply of maternal antibodies to it, which can only be achieved by delivery.
Delivery with Rh-conflict
Unfortunately, with Rh sensitization, it is often necessary to carry out the delivery ahead of schedule, because on the later dates pregnancy, there is an increase in the number of antibodies that go to the fetus.
Depending on the condition of the fetus and the duration of pregnancy, the method of delivery is individual in each case. It is believed that a caesarean section is more gentle for the fetus, and therefore, in severe cases, it is resorted to. With a satisfactory condition of the fetus, gestational age over 36 weeks, in a multiparous woman it is possible to conduct labor through the vaginal birth canal with careful monitoring of the fetus, prevention of intrauterine hypoxia. If his condition worsens during childbirth, the management plan may be revised in favor of a caesarean section.
Forecast for Rh-conflict
The prognosis depends on how early Rh immunization was diagnosed, on the value of the antibody titer and the rate of its increase, as well as on the form of hemolytic disease of the fetus. The earlier antibodies are detected in the mother's blood, for example, at a period of 8-10 weeks, the more prognostically unfavorable it is. A rapid increase in antibody titer, titer above 1:16, early detection of it (at periods less than 20 weeks) is the basis for an unfavorable prognosis. In such cases, not only the risk of hemolytic disease of the fetus increases, but also the risk of miscarriage.
The most prognostically unfavorable form of hemolytic disease of the fetus is edematous. Such children often require treatment in the conditions of the pediatric intensive care unit and intensive care, replacement blood transfusion. The most prognostically favorable form is the anemic form, (depending on the severity of the anemia). In the icteric form, the determining criterion is the level of bilirubin. The higher it is, the higher the possibility of affecting the central nervous system fetus, which is manifested in the future by dementia, hearing loss.
Prevention of Rh-conflict
Currently, in order to prevent Rh sensitization, human anti-Rhesus immunoglobulin D is used. This drug has proven efficacy and exists under several trade names, such as: "HyperRow C / D" (USA), Resonative (France), anti-Rhesus immunoglobulin D (Russia ).
Prophylaxis should be carried out during pregnancy at a period of 28 weeks in the absence of antibodies in the mother's blood, since it is during this period that the risk of contact of the mother's antibodies with the fetal erythrocytes increases sharply, and therefore the risk of hemolytic disease of the fetus also increases. Due to the administration of the drug, an antibody titer may appear in the blood, therefore, after the administration of the drug, the determination of antibodies is no longer carried out. Further, the prophylaxis should be repeated within 72 hours after childbirth in the event that the patient is planning the next pregnancy. If bleeding occurs during pregnancy, as well as during cordo- or amniocentesis, as well as in the postpartum period, the administration of immunoglobulin should be repeated, because Rh sensitization may occur during the next pregnancy in response to the entry of fetal blood (with bleeding from the placenta vessels) into the mother's bloodstream.
Also, prophylaxis with an injection of the drug should be carried out for any outcome of pregnancy: miscarriage, medical or instrumental abortion, ectopic pregnancy, vesicular drift within 72 hours after termination. Particular attention is paid to blood loss, with the appearance of which the dose of the drug should be increased.
Obstetrician-gynecologist D.V. Kondrashova






